
Harnessing Social and Digital Media to better reach vulnerable populations
This project is developing a toolkit for MSF teams to harness social and digital technologies to better reach vulnerable displaced populations that face barriers in accessing health care.
Tell us about the problem you are trying to solve.
Vulnerable populations face various barriers in accessing healthcare. Some of these barriers can be physical – for example, when a natural disaster or violence blocks the way to health care services, or when people are on the move and do not come across a health facility on their route. But some of the barriers to access and proximity are socio-cultural – for example, spiritual beliefs or mistrust in health care providers, which prevent people from seeking help.
At the same time, access to communication channels, internet, and social media is growing among MSF beneficiaries every day. New media technologies and social networks offer opportunities to rethink and explore the way MSF provides care and reaches populations who otherwise lack access to health services. Multimedia channels can bring MSF closer to the people, to support them even when we can’t be physically present, and to build a relationship where we can exchange information in familiar virtual spaces.
What is your solution? What motivates you to work on addressing this problem?
We are exploring how we can use existing social networks and digital media to improve the quality of care and increase operational efficiency. The deliverables of this 18-month project includes a toolkit for field teams on how to use new media to engage with communities as a complementary operational strategy.
The video below summarizes the ambition of the project:
The toolkit follows five key steps:
- Setting our goals – In the first phase, we are prioritizing operational challenges and goals with our coordination teams on the ground. For example, new media can be used to increase the patient cohort or to communicate with specific population groups.
- Understanding our audience – Understanding is key. What access to channels do people have? What are their concerns and aspirations? How do they currently communicate and share information? And who are the trusted information sources in the community?
- Identifying the right solution – By understanding the current habits and needs of community members, we can select the right channel, the right type of content, and the right messages to reach people in a way they can relate.
- Planning operations – A risk analysis needs to be done, a monitoring plan set up, and human and financial resources planned.
- Content creation and implementation – Time to get creative! Digital channels allow for new types of engaging content including videos, animated GIFs, audio messages, live broadcasts, songs, graphics, etc. During implementation, teams are continuously measuring the impact both online and offline and adjusting the strategy when needed.
In summary, the multimedia strategy must be created in a way that people feel included and represented through a familiar channel, while simultaneously monitoring and responding to operational goals.
What have you done so far and what results have you achieved?
A first version of the toolkit is currently being used in Colombia and Mexico. Multimedia strategies for the two countries have been created and we are continuously learning and adapting the tools during implementation.
The starting point of the strategy is driven by operational priorities. When COVID-19 hit our MSF missions, pandemic-related community engagement, health promotion and service promotion became an important objective of our multimedia strategy. After an analysis of the commonly used channels and societal structures, the teams in Colombia and Mexico defined the best ways to interact with their populations.
We are now connecting and sharing information with community leaders through WhatsApp, airing health promotion messages and a COVID-19 song on local radio stations, and reaching younger audiences through Facebook campaigns. MSF GIFs are circulating to promote the COVID-19 support line. An animated game has been developed to debunk myths and rumors. And in a Facebook live Q and A, MSF doctors explain the ins and outs of COVID-19 and how to prevent it.
Topics change as the pandemic evolves, and as new needs and challenges arise. Current activities are related to the stigma faced by COVID-19 patients, stigma faced by health care staff, the increase of sexual violence due to self-isolation, and the mental health implications of the outbreak for adults and children.
Below are some examples of the content being shared with our populations:
Salsa Corona song – shared through WhatsApp, Facebook, local radio and television:
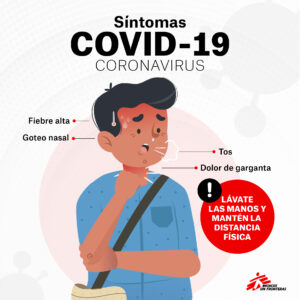
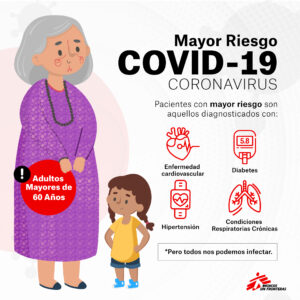
Infographics, audios and videos are shared with patients, migrant shelters and other actors through Whatsapp:
A Facebook campaign on myths and realities:
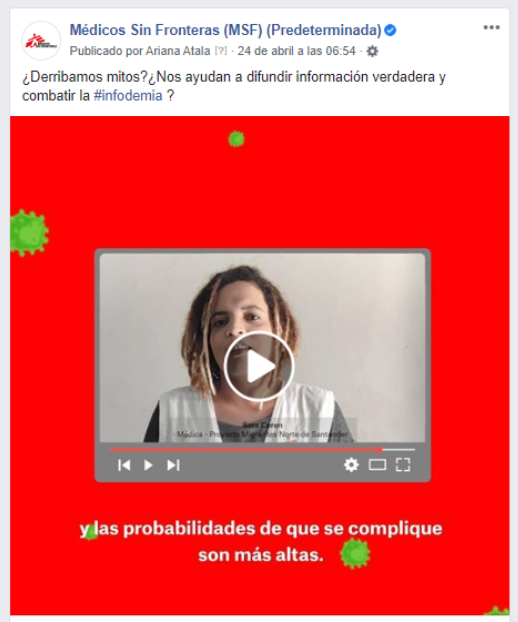 |  |
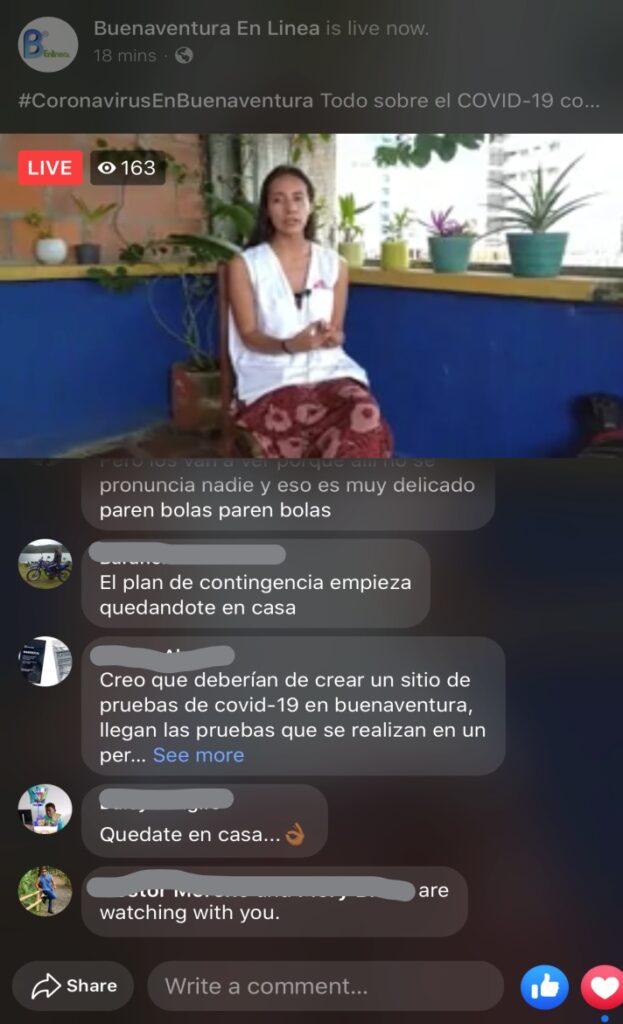
A Facebook Live session with and MSF doctor through a local page received over 13,000 views:
Two GIFs to promote the mental health support line:
 |
How has your project pivoted to support MSF’s response to the COVID-19 pandemic?
Information is key to limiting the spread of the COVID-19 virus and when traditional methods for health promotion like community meetings and door-to-door visits are not feasible, digital community engagement can be a solution to inform, communicate, interact, and engage with mass audiences while staying safe.
During the pandemic, a new COVID-19 community engagement and dissemination support team was set-up to work with Operational Center Barcelona missions worldwide. The lessons learned from this TIC project and the implementation in Colombia and Mexico are being transferred to different continents, and we have engaged with 20 missions to date.
The support team brings together the Communication and Health Promotion focal points of each mission, to brainstorm together on the best strategies to reach key populations. We are shifting the thinking from meetings and radio to WhatsApp and Facebook, from posters and flyers to audiovisual content, and from ‘messages to all’ to messages and channels for specific target groups. The support team works hand-in-hand with the Health Promotion referent, Operational Comms and a Creative Team dedicated to the development of materials for the missions. Below are just few examples created by the team and used in several missions.
- GIFs on common myths, made in French, English, Spanish and Arabic – shared through digital media across mission around the world.
- Visuals targeting kids, explaining preventive measures.
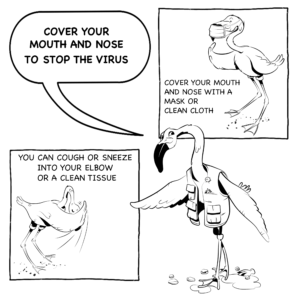 |
What challenges have you faced? What lessons have you learned? What is next?
Using channels like Facebook or Telegram are not the first thing a team thinks about when tackling an operational challenge. As it is not part of any standard operational procedure (yet), a portfolio of examples must be developed to demonstrate that new media is not just a nice to have, but that it truly contributes responding to real challenges that our teams are facing in the field. The COVID-19 pandemic has accelerated this process and has shown us the power of using new media and tapping into existing social infrastructures in a variety of contexts. A next important challenge is to see how we can best integrate this into MSF’s ways of working, so that every project can consider this avenue from the start.
What have staff said about the project?
“In the midst of the response to COVID-19, this project has allowed us to explore and take advantage of alternative channels to communicate with the communities with which we work, helping us to overcome the barriers imposed by the isolation measures, and allowing us to have contact with a number of important people.”
– Daniel Macía Agudelo, Deputy Medco, Colombia
“The multimedia strategy supports the mission’s medical operations. COVID-19 related, the health promotion material and distribution of important topics for coronavirus patients and their family members has contributed. The strategy also included the promotion of a mental health telephone line, for a population that does not have access to mental health care otherwise. It is and should be a support tool for medical operational activities.”
– Nestor Rubiano, Mental Health Referent, Mexico
“In the COVID context, where social distancing is a mandatory premise for our operations, the TIC project activities give an opportunity for a new dimension to the scope of our activities.”
– Sergio Ferrer, Fieldo Buenaventura project, Colombia
“The materials that were made within the multimedia strategy are very useful because they guide the community in a simple way, clearly explaining the support MSF can give. They are a simple, clear and objective materials, using community language.”
– Jonathan Prieto, PMR Guerrero Project, Mexico
“The TIC project in Colombia constantly surprised me with its creativity and capacity to respond to the health problems that surround us. The COVID-19 outbreak here has brought out some dangerous aspects of social media – fake news and misinformation – with a real threat of damage to the populations where we work. This project gives us the tools to respond to these threats on equal terms.”
Steve Hide, Head of Mission, MSF OCBA, Bogotá, Colombia
Are there any interesting partners that you are collaborating with?
Community members are our key partners! Their preferences and habits define the type of channels and content that are being used. By identifying and collaborating with the community gate-keepers, MSF can spread messages beyond our own networks. Think village elders, teachers, local artists, and adolescents with big online networks. In Colombia, audiovisual COVID-19 materials are being shared with community leaders in WhatsApp groups, who then further share the content with people in their own neighbourhoods.
In Mexico, we have seen how other actors are key to reaching a wider group of beneficiaries. Infographics have been shared through WhatsApp with 100+ NGO’s and migrant shelters along the migration route across Mexico. Many of them then further share the content through their own channels. We’ve seen MSF content shared on the Facebook channels of our collaborators, and we’ve even come across printed versions that have been hung in migrant shelters. This was unexpected learning for the project: to see content move from offline to online and back to offline again! In Colombia, MSF materials reached a schoolteacher via WhatsApp; he then printed the materials and hung it in school to show his students. This is another example of how digital channels and social networks can spread engaging content, which can then be adapted to the needs and preferences of the population.
 What is the expected long-term impact of the project? How will this project improve MSF’s lifesaving work?
What is the expected long-term impact of the project? How will this project improve MSF’s lifesaving work?
If we can integrate the use of new media as a standard option to reach operational objectives, there is huge potential for broader impact. Service promotion can for example lead to more consultations for survivors of sexual violence within 72 hours or to increased turnout at a measles vaccination campaign or a distribution day for non-food items. Engaging health education can lead to improved health-seeking behaviour, better implementation of preventive measures, and increased adherence to treatment and care. We can access groups that we couldn’t reach before, share information with high numbers of people at the same time. Moreover, beneficiaries can also reach MSF to ask questions about their health, express their needs, and provide feedback on our programs. This can ultimately help MSF to design more inclusive projects.



