
Transforming clinical care at the patient’s bedside with point-of-care ultrasound
In remote and low-resource settings, point-of-care ultrasound (POCUS) is transforming the quality of care delivered at the patient’s bedside. By using real-time information, POCUS empowers frontline health care providers (including nurses and midwives) to better treat patients in need of trauma, obstetrics or emergency care.

Tell us about the problem you are trying to solve.
Clinicians in our field-sites have limited access to diagnostics. This often affects their ability to care for and treat our patients, which is frustrating for patients, their families, and our staff. Point-of-Care-Ultrasound (POCUS) takes diagnostic technology – in this case a portable ultrasound machine – to the bedside in the field, so clinicians themselves can answer important diagnostic questions in real-time to guide patient management. For many clinical experts, these portable machines, which are about the size of a laptop, are like the revolution of the stethoscope. With some basic training, clinicians can literally see inside the body, and more rapidly diagnose what might be going on.
Imagine the following situation that is quite common in MSF field sites: there has been a horrible traffic accident. The patient that is brought to the ER has bleeding wounds, but the clinicians are not sure if his abdominal organs were hurt as well, which might require immediate surgery. For now, he seems stable, but will this last? In any scenario, this patient will need close observation. If POCUS is available, the clinicians can do a quick exam with the ultrasound machine. In less than 5 minutes they will know if there is bleeding present in the patient’s belly or chest and can act immediately. Often, this rapid diagnosis helps save lives.
In this way, POCUS solves several problems. It empowers clinicians who might otherwise have limited capabilities in their field hospital to assess patients better, and more quickly. It narrows the time to make the right diagnosis and initiate potentially life-saving treatment. And it allows the medical team to change the plan of care, which may include transfer to another facility or surgical consultation. This often improves patient outcomes, which is always the basic goal of our work!
What is your solution and what motivates you to work on addressing this problem?
Our solution is to train MSF field clinicians how to use and integrate this technology in a sustainable and useful way to improve patient care.
We’re motivated both by seeing the patient outcomes, and the gratitude our field clinicians have when they have a useful diagnostic tool.
Many of our national staff clinicians lack access to training with novel diagnostic tools. They hear and read about this technology, but due to resource limitations in the countries where they live and work, they often don’t have the opportunity to integrate this knowledge into their clinical skills. Teaching POCUS gives them a life-long clinical skill which is a game changer. It adds a low-cost, safe, radiation free method for helping them make life-saving diagnoses.
Ultrasound machines have been around for many years, typically performed by specialist radiologists or obstetricians. In the last 10 years, general clinicians – everyone from midwifes to emergency doctors, realized there was a way to simplify imaging examinations which help bedside clinicians solve common clinical problems. Ensuring our clinical staff at MSF are learning the same skills as young trainees in other countries is extremely important.
The biggest motivation is hearing our clinicians tell us how POCUS improves patient care. Those real-life testimonials keep us going:
- The midwife who identified an expectant mother with a high-risk pregnancy complication and refer her on time for a c-section.
- The Clinical Officer who determined a child has a dangerous fluid collection in their lungs from a complex pneumonia and got them the procedure and treatment they need before it was too late.
- The Physician’s Assistant who diagnosed that an older woman’s cough was actually from a dangerous heart condition, not a lung problem like other clinics thought.
- And the surgeon who struggled to understand the cause of swelling in a young girl’s calf and saw instantly that what she thought was a simple skin infection is actually a deep pocket of pus that needs surgery.
We are motivated by our clinicians feeling they have the tools to take good care of their patients.

What have you done so far and what results have you achieved?
While ultrasound has been used in MSF projects for many years, mostly in obstetrics, this newer concept of integrated POCUS trainings only started several years ago.
Just since 2018, more than 22 countries have received POCUS implementations, and more than 45 separate projects have trained staff. We’ve trained nearly 500 clinicians from various levels and backgrounds (midwife, clinical officers, physicians assistants, general practitioners, specialist MDs), and more than 90% of these clinicians are from the countries where we work, instead of short-term expat staff. In addition, we’ve instituted a train-the-trainer model, so some of our former students have now become POCUS trainers themselves for other staff in their country.
We piloted a new full-time position for one of our South Sudan clinicians to be the POCUS leader and coordinator for his country. He serves as a clinical POCUS trainer and focal point for POCUS integration into our many projects sites in South Sudan. Building local and regional capacity is key to long-term sustainability of POCUS, we hope to replicate this position and model in several other regions worldwide.
In addition to field training, we are conducting multiple Operational Research projects to evaluate how POCUS fits into the clinical algorithm for conditions such as paediatric tuberculosis, COVID, and sepsis, with more research planned in the coming years.
Support from the MSF telemedicine platform is essential when our field teams have complex clinical cases and ultrasound images they need help interpreting. We’ve collaborated with the Telemedicine team to ensure we have over 20 world-renown POCUS experts available to help our clinicians answer complex questions 24/7. Our volunteer POCUS experts on the Telemedicine platform provide crucial expertise for field teams treating the most complicated patient cases.

Finally, we are constantly testing new ultrasound technology, whether it’s smaller machines that plug into smartphones, or novel uses of Artificial Intelligence – to make sure our clinical teams at MSF have access to the most innovative ultrasound tools.
What have staff said about the project?
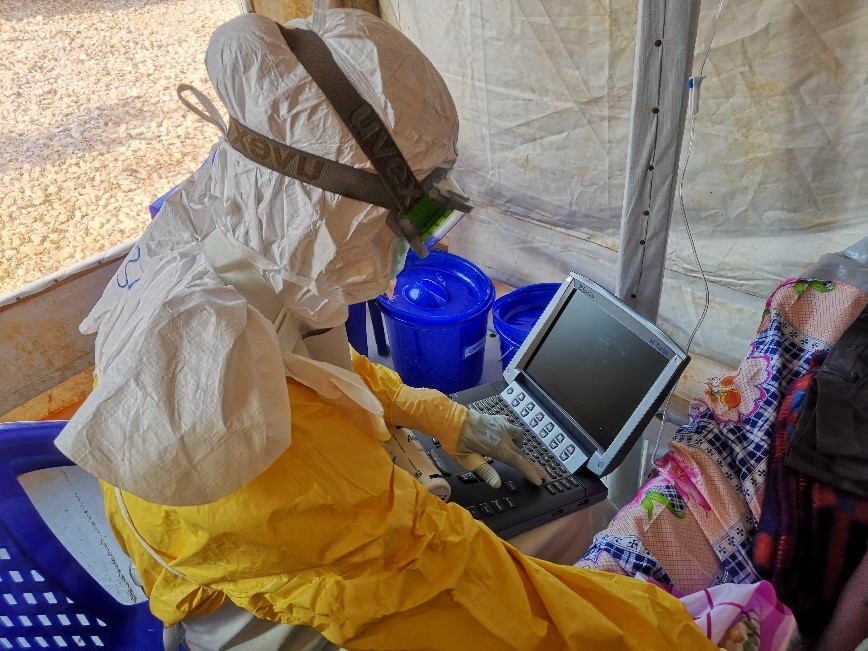
“POCUS is very essential in our work as clinicians. Because it gives us a quick narrow differential diagnosis, provides immediate feedback about the case and also reduces the complication rate during procedures. So, it improves the clinical outcome.”
Akram Abdalbaki Ahmed Qassim, MD, Yemen (pictured below)

“I remember when I received a child of 9 years in the dressing room with a swelling of the left calf. He was referred from the health post because of an abscess for incision and drainage. Before the procedure we decided to do a soft tissue ultrasound first to verify. During the scan we found cellulitis and no abscess of the calf. We removed the child’s cannula and cancelled the procedure, started i.v. antibiotics and after 5 days the child was completely cured without any abnormality.”
– Meshack Kasitu, CO, Tanzania
“We have 2 departments in our hospital where we use POCUS. In the emergency room it is used to diagnose emergency cases, especially trauma cases. In the paediatric ward where I am working, we use POCUS very often for the diagnosis of lung diseases.”
– Ghassan Marie Hasan, MD, Iraq

“POCUS training gives staff important skills that are transferrable to any health care setting, and therefore will continue to make a positive impact long after MSF has left. It makes long-lasting, tangible differences in the countries where MSF works.”
– Dr. Susie Broughton, MSF MD
“I didn’t realize how fast the staff would pick up POCUS when I went to Liberia as their POCUS trainer. Their passion and enthusiasm was unlike any students I have ever trained, and it raised their confidence in clinical decision making after a few weeks.”
– Dr. Rupa Narra, MSF MD and POCUS trainer

How has your project pivoted to support MSF’s response to the COVID-19 pandemic?
Our primary concern is the safety of our patients and staff. As such, we immediately developed Infection Prevention Control educational materials specific to ultrasound machine use in the COVID-19 pandemic and are available for site-specific advice.
POCUS has been shown to be useful in COVID-19 care in high resource settings. Similar to x-ray, while it can’t single-handedly ‘diagnose’ COVID-19 (only lab tests can), there is a characteristic pattern of disease seen on lung ultrasound in COVID-19 patients. POCUS can also help determine if there are other comorbidities making the patient sick, such as cardiac dysfunction. In many countries, POCUS has been integrated into different parts of COVID-19 clinical algorithms. Our role is to help MSF decide when, where, and if to integrate POCUS into COVID-19 care.
To meet this need, we developed specific curriculum for our POCUS-trained sites, to help educate our clinicians about COVID-19 findings on ultrasound.
Our South Sudan regional POCUS trainer was selected to be part of the South Sudan COVID response team, where he was responsible for medical related activities and development/conduction of trainings.

We developed several novel training and research projects to better understand the role of POCUS within MSF COVID-19 projects. Our team piloted a training in Italy for POCUS use in home-based care, which is ready for research should a second wave occur. This assesses how clinicians could take small handheld ultrasound machines into patient’s homes and evaluate them at home for concerning symptoms. We also currently have a POCUS in COVID-19 operational research project underway in coordination with Hospital del Mar in Barcelona. This exciting study allows us to collaborate with a top-level hospital to evaluate how ultrasound findings may predict severity of COVID-19 symptoms – in relation to a variety of lab and clinical markers.

In addition, we’ve had to adapt and pilot new ways to carry out POCUS training in an era with limited travel. We’ve piloted a remote training-of-trainers and field training in several key sites, to map out the unique challenges with these models. Digital and distance learning requires rethinking the way we approach clinical education, and we’re tackling that challenge daily.
What challenges have you faced?
Successful integration of POCUS into MSF projects requires high-quality longitudinal learning programs. Think of it like learning a new language. Even after you do the “intensive training month”, you need constant practice and communication with your instructor until you become proficient in the language.
Even though it is challenging, our ‘trainings’ are really long-term mentorship programs with the clinical staff in site. That’s part of why they have ‘follow-up’ trainings after several months – to check and build their skills.
But realities in the field are changing constantly, and reliance on expat POCUS trainers is not sustainable to continually train the rotating clinical workforce in our project sites. To mitigate this, we have developed a train-the trainer model. All our field-implementations have a goal of training several clinical staff as the eventual POCUS ‘superusers’, and then trainers. This allows the clinical staff in the site to develop their capacity as mentors for their fellow staff. Becoming a good facilitator is not learned overnight. We piloted the concept of local trainers last year and learned a lot. This year, we are developing a training-of-facilitators course to provide our clinical trainers with the practice and skills they need to facilitate POCUS training and integration well.
Most of our field-based trainings in 2020 had to be cancelled, delayed, or rescheduled due to COVID-19 travel restrictions. However, in light of reduced travel, it’s created an opportunity for our previously trained national staff colleagues or expat colleagues in the field to rise to the challenge and become POCUS trainers with our remote support. Again – this process has helped us learn how to develop a strong training-of-facilitators program. We believe POCUS is best taught in-person and at the bedside, which has become difficult in 2020. Despite this, we’ve managed to adapt several models which allow our local staff to still learn this vital skill. It has also pushed our program to assess the digital and online POCUS education content that exists and evaluate what is most pertinent to our MSF learners.

Are there any interesting partners that you are collaborating with?
We received the POCUS Academy 2020 Mission POCUS Grant, https://www.pocus.org/missionpocus/, to pilot their POCUS certification exams with several of our national staff POCUS clinicians. This will evaluate the possibility of integrating formal internationally recognized POCUS certification into our education and training processes. National staff colleagues from 7 different countries will have the opportunity to be independently evaluated by taking these exams, but then also give valuable feedback on their adequacy and relevance to MSF project sites.
Because we are interested in the online learning/evaluation software available, we also began working with ImageSim (https://imagesim.com/) an online competency-based learning system. These online POCUS modules test students’ abilities to correctly interpret hundreds of real cases – matching the clinical symptoms to their ultrasound findings. We hope to integrate these learning modules into our training programs.
What is the expected long-term impact of the project? How will this project improve MSF’s lifesaving work?
The project has impact in two main realms: field staff capacity building and improving patient care. We believe the two go hand in hand.
In the long-term, we aspire to have POCUS well-integrated into many, if not most, MSF projects. The integration is key, to ensure staff use it appropriately, with good clinical skills and decision-making, to make more accurate more rapid diagnoses in the specific medical conditions where POCUS is most useful. The use of POCUS in resource-limited settings is still relatively new, meaning we may find it has the biggest impact in different patient scenarios than in Europe or Canada, for instance. In this way, MSF’s work in this realm is helping inform countless other POCUS educators worldwide.
By focusing on training the national staff based in the countries where we work, they gain lifelong clinical skills with an important integrative technology. Empowering local leaders and facilitators gives them additional tools that allow them to transfer skills to others throughout their careers. This sustainable development that doesn’t rely on expat or ‘headquarter’ based specialists is key to transferring skills where they are most needed.
Having staff trained is one piece of the puzzle. The other is evaluating how POCUS impacts, and hopefully improves, patient care. To do this well, we evaluate in which situations POCUS is really a game-changer, and how the patients and staff feel about the use of POCUS during clinical care.
Our research projects, the coordination with the Telemedicine platform, and the continuous integration of novel POCUS technology will help long-term integration of POCUS into MSF projects to improve clinicians’ diagnostic abilities, and ultimately patient care.
At the end of the day, if both our clinicians and patients benefit, we’re on the right path.



